Minimum Requirements for the Interoperability of Special Operations Surgical Teams
An Assessment Based on Current National Standards and NATO Doctrines
Frank Klemmer
Abstract
Background
To reduce mortality and morbidity in combat situations, a Special Operations Surgical Team (SOST) should be positioned close to the point of injury (POI). SOST capabilities include both damage control resuscitation (DCR) and damage control surgery (DCS) performed by specially trained medical professionals. The modern battlefield requires mobile, lightweight, scalable, modular, and flexible surgical capabilities like SOST to meet established casualty care timelines in medical support of Special Operations Forces. There is currently a shortage of SOSTs capable of DCS and DCR, which must be addressed through the establishment of minimum requirements at the NATO level via the development ofnational medical standards and targeted training programs.
Method
To establish the minimum requirements for interoperability, a mixed-methods approach was utilized. The Bundeswehr's Medical Service hosted the SOST international working group in Munich in September 2024, where 72 participants from 13 nations and 15 Special Operations Surgical Units were organized into 4 syndicates. Discussion within the syndicates focused on Selection and Training, SOST Platforms and Configurations, DCR and DCS capabilities, and SOST Evaluation Methods. Following the workshop, feedback was solicited from Subject Matter Experts (SME) representing all 13 nations regarding team configuration, platform variants, and SOST skills. The process ensured a comprehensive understanding of interoperability and minimum requirements through both quantitative and qualitative (Delphi-Method) methods. Additionally, literature research was conducted in NATO documents to highlight previously established guidelines.
Results
The analysis of 15 quantitative responses (15 questions within the syndicates) and 39 qualitative responses (from each nation) regarding Selection and Training, SOST Platforms and Configurations, DCR and DCS capabilities, and SOST Evaluation Methods resulted in insights that highlighted commonalities among the nations. Minimum requirements for working in the international environment of NATO have been identified and listed as prerequisites.
Conclusion
The shared insights among nations and syndicates regarding Selection and Training, SOST Platforms and Configurations, DCR and DCS capabilities, and SOST Evaluation Methods indicate that foundational data for establishing minimum NATO requirements is available. The data shows a wide variance in SOF medical capabilities across multiple NATO countries supporting the need for formalized NATO doctrine focused on a standardized approach to medical interoperability.

1. BACKGROUND
The necessity of maintaining a Special Operations Surgical Team (SOST) within the rescue chain in special operations is supported by NATO doctrine and directives (References in the Endnote). However, the minimum requirements and configurations are not defined and interoperability within NATO is not specified. The current and future operational environment will require mobile, lightweight, scalable, modular, and flexible surgical capabilities to meet doctrinally accepted casualty care timelines (Transfusion, 2024, Tägerwilen II Report)i.
To reduce mortality and morbidity in combat situations, it is essential to position SOSTs close to the point of injury (POI). SOSTs provide critical capabilities in damage control resuscitation (DCR) and damage control surgery (DCS), delivered by medical professionals who have undergone selection and specialized training. The requirements of the modern battlefield necessitate skills that traditionally trained medical providers do not receive. These skills include both tactical and medical knowledge. Without adequate training and selection of team members, SOST forces can be a hindrance the mission rather than a risk mitigation tool and lifesaving asset.
Despite their importance, there is currently a shortage of SOSTs capable of providing DCS and DCR for special operation forces (SOF). This deficiency must be addressed through the establishment of minimum requirements at the NATO level, which can be achieved by developing national medical standards and targeted training programs. The need to maintain a SOST within the medical evacuation chain in special operations is emphasized by multiple NATO doctrines; however, medical minimum requirements, technical implementation of platforms, and team configurations remain undefined. Furthermore, interoperability among NATO member nations regarding SOST capabilities has not been specified, leading to discrepancies in deployability and effectiveness.
The contemporary operational environment is characterized by rapid changes and an increased operational tempo, further underscoring the need for effective and responsive medical support. Such qualities will ensure that SOSTs can provide immediate assistance in high-stress and hazardous environments with varying operational demands.
Currently, the evaluation and validation of SOSTs are hindered by the limitations of NATO's evaluation doctrine, which begins only at Role 2 B. There are no parameters to evaluate and validate SOSTs. Which does not fit conveniently into the Role 2 category due to the high mobility and limited holding capacity SOST forces provide. This gap has contributed to a significant deficit in the establishment and operational readiness of SOSTs within NATO.
The lack of comprehensive guidelines and minimum requirements hinders uniformity in SOST configurations, leading to significant diversity in team compositions and specialized training programs that are difficult to compare due to differing standards and educational pathways. Additionally, team sizes within SOSTs range from 3 to 10 members based on operational context, which complicates coordination and integration among allied forces and may undermine the effectiveness of medical interventions in combat situations. This variability poses challenges to NATO's medical interoperability and flexibility.
2. METHOD
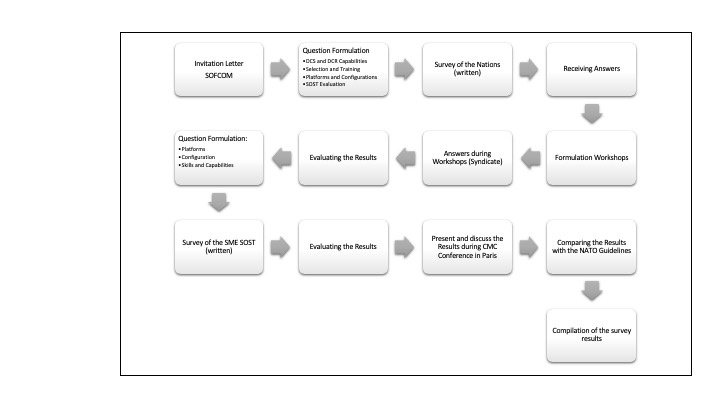
The national contacts and SOST members were invited to the Munich working group, where they were divided into various syndicates to discuss the four key themes (1) DCS and DCR capabilities (2) Selection and Training (3) platforms and configurations, and (4) SOST evaluation.
The individuals from each nation were assigned to different syndicates in order to minimize the influence of group pressure (national opinion) and the dominance of individual persons (superiors).
The results from each syndicate were summarized and sent to subject matter experts from each of the 13 nations for analysis and review (Modified Delphi – Method).
The four key themes were assessed and analyzed for minimum SOST requirements.
The key themes as follows:
- DCS and DCR Capabilities
- Selection and Training
- Platforms and Configurations
- SOST Evaluation
The key themes were used as a basis during the workshops, where 15 SOST (or similar representatives) from 13 nations answered a total of 17 questions. During the syndicate work, a combination of standardized questions, focus group surveys, and a modified Delphi method was employed. A consensus of ≥90% was reached for 14 statements. In parallel, responses were requested by having the SME SOST fill out an Excel sheet with identical topics. Responses with an average score of >90% were included in the following investigations of commonalities and interoperability.
3. COMMONALITIES AND INTEROPERABILITY
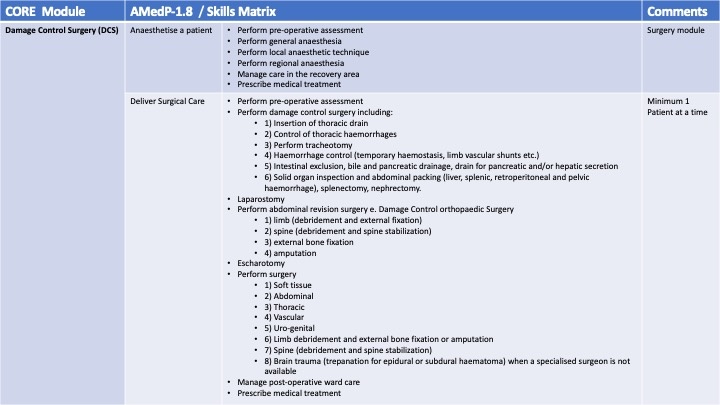
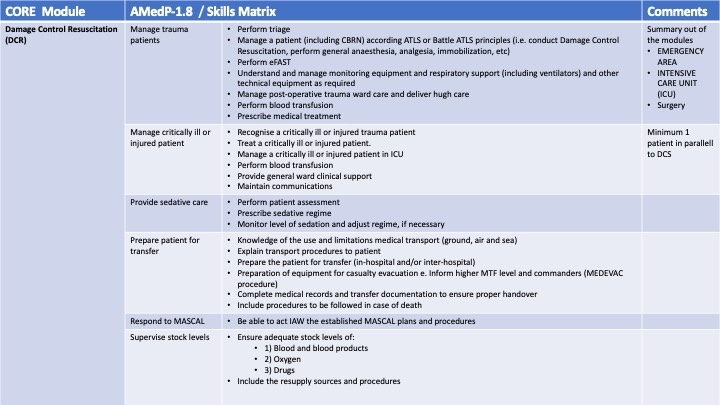
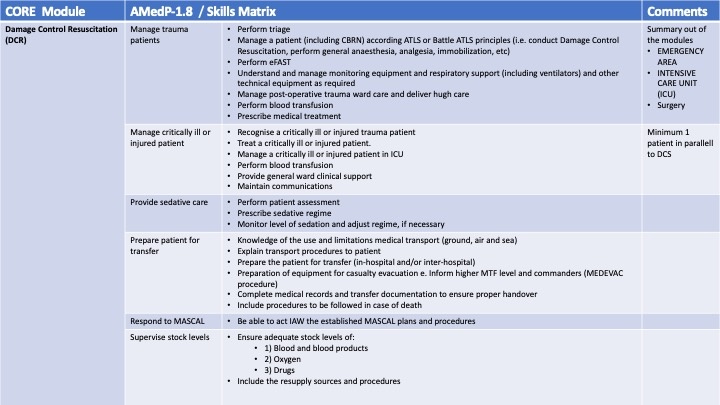
3.1. DCS and DCR capabilities
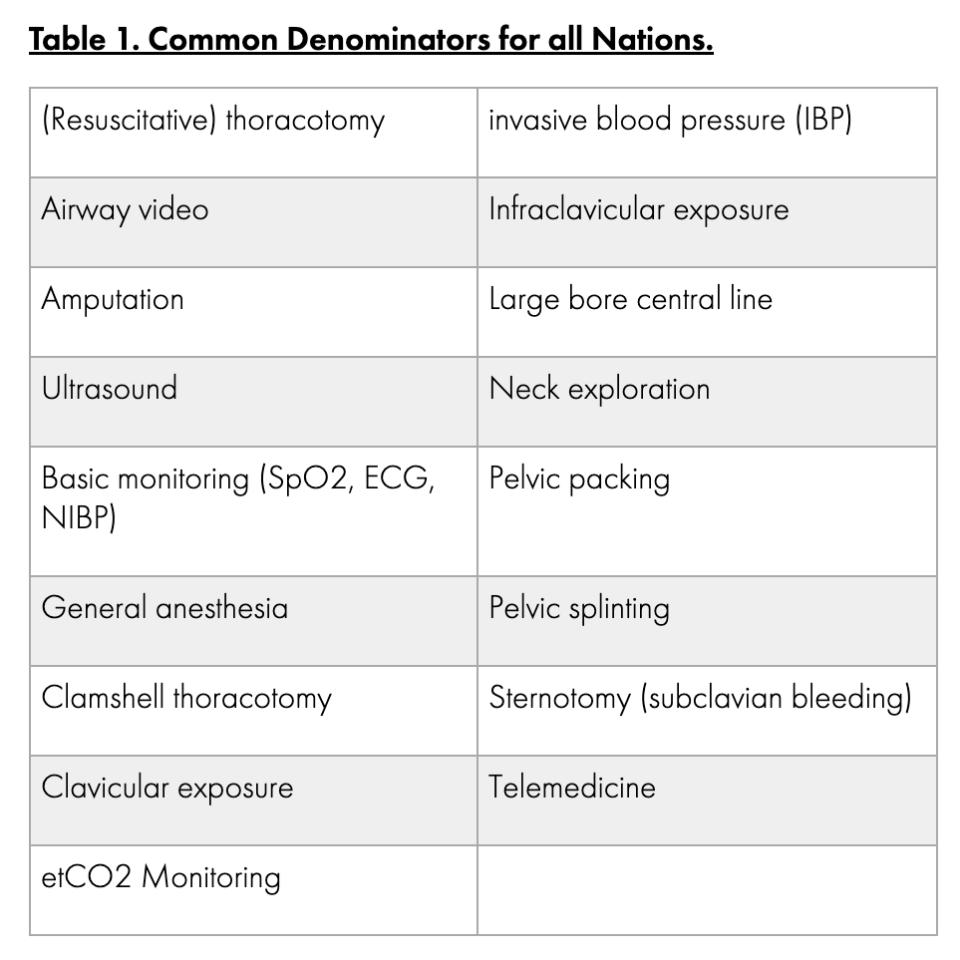
SOST must be able to provide damage control resuscitation, damage control surgery laparotomy/thoracotomy, field anesthesia, amputation completion, and vascular shunting. These results are consistent with the guidelines of the NATO Special Operations Medical Leaders Handbook (2016)ii. The current version of the Handbookiii (2024) was not considered here, as it does not reflect the SOST requirements but rather aligns more with a conventional Role 2 forward (R2F) approach. To list some differences, the SOST has only limited patient holding capacity, limited resupply, and no prescribed structural configuration due to platform independence. Additionally, unlike conventional R2F, SOST can be deployed in land, air, and sea domains due to their materials, training, and platform independence.
Through the survey of the international SME SOST, the following skills and capabilities were identified as common denominators for all nations. Out of 49 selected skills and competencies, 17 shared a commonality among all SOST.
3.2. Selection and Training
Requirements for Training and Education by NATO Doctrine: For interoperability, a minimum of Language Proficiency Level (LEVEL 2)iv in English with specialized training in medical English is required. Due to the operational environment of SOST, a classification into the training level of SURVIVAL, EVASION, RESISTANCE, EXTRACTION (SERE) at LEVEL Bravov is required.
Selection: SOST personnel is selected based on their physical and mental fitness, medical competence, psychological profile and mindset, as well as their adaptability to the tactical environment of the Special Operations Forces.
Training: The foundation for the tactical training of SOST must be defined by the national Special Operations Forces, and the content must be conveyed in the basic SOST training. Additional training in Special Operations Medical Planning and Support should be integrated into the program.
An interesting aspect here was the national necessity in training courses such as diving medicine, altitude medicine, parachuting, fast roping, and tropical medicine. This was only sporadically supported by nations as required training. However, it raises the discussion point of which training courses should be considered minimum requirements for a NATO SOST.
The summarized training content must continuously be practiced as small unit tactics in large-scale military operations at the national SOF level and within the NATO SOF environment.
Key Requirements Due to the increased implementation of minimally invasive procedures and computer-assisted surgeries, a national system must be established to ensure training for wartime surgery, as most clinics in Europe cannot achieve the case numbers for gunshot and stab wounds like the extensive civilian trauma network within the United States or specific hospitals such as Chris Hani Baragwanath Hospital, South Africa.
3.3. Platforms and Configurations
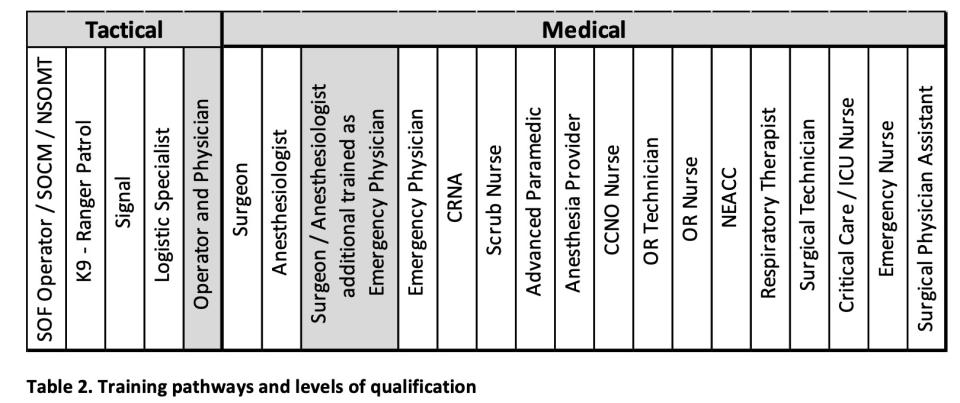
Configurations: The team configuration of a SOST for establishing a surgical workspace (1 patient at a time) consists of 6 individuals for 90% of respondents or can be reduced to 6 individuals due to team size. A fixed assignment of specific job descriptions is not possible, as 20 different training pathways and levels of qualification have been described. The areas represented in gray show the dual function, tactical and medical, as well as the dual training as a special feature in the SOST.
PLATFORMS:
SOST must be able to reach the operational area on foot and be deployable on platforms such as van, truck, tent, house, and ship. These options of the platforms have been confirmed by 13 SOST or comparable surgical elements and are already implementable by the nations. The rotary wing and fixed wing variants must be implemented; however, there is a lack of approval for the SOST systems from the aviation safety authorities of the countries, which affects interoperability. Deployment on aircraft must be authorized repeatedly by the responsible military authorities and cannot be generally planned as a standard size.
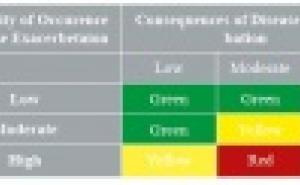
3.4. SOST Evaluation
As a working basis, the documents and doctrines were summarized: The Law of Armed Conflict – ICRC, STANAG 6001 – Language Proficiency Levels, AMedP- 1.8 Skill Matrix, AMedP – 1.6 Medical Evaluation Manual, Medical SOF Evaluation (SOFCOM), and AMedP – 4.13 NATO Special Operations Forces (SOF) Medical Support. The individual requirements were discussed and evaluated. The two main statements were:
- An evaluation form provided by SOFCOM is necessary to define the minimum requirements for NATO SOST.
- The SOF Eval must be close to the evaluations of conventional medical treatment facilities in the areas of Damage Control Resuscitation (DCR) and Damage Control Surgery (DCS).
The evaluation / validation must not be limited to paperwork but must also be conducted through practical implementation/exercises.
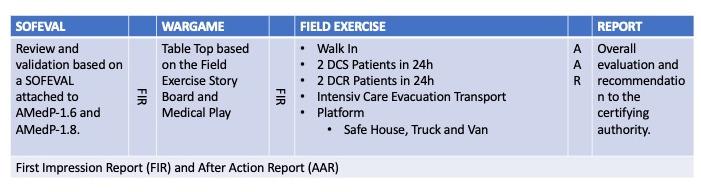
The process outlined in the table is based on the principles of the NATO Course International Military Medical Observer and Trainer Course and the International Military Medical Evaluator Course.
4. CONCLUSION
The data determined in the current NATO doctrines, NATO requirements, and four thematic areas highlight the existing commonalities in SOST and thus provide a standardized approach to interoperability that should be formalized in NATO doctrine as a minimum requirement.
5. ACKNOWLEDGMENTS
All members of the SOST Working Group (Munich) and the national Subject Matters Experts SOST are acknowledged for their contribution to these recommendations.
6. REFERENCES
i Christian Medby, Colleen Forestier, Benjamin Ingram, et al: The Tägerwilen II report: Recommendations from the NATO Prehospital Care Improvement Initiative Task Force, 3.3 Forward surgical capabilities, Transfusion, February 2024, https://doi.org/10.1111/trf.17760
ii NSHQ: NATO SPECIAL OPERATIONS MEDICAL LEADERS HANDBOOK, Chapter 8, June 2016
iii NSHQ: NATO SPECIAL OPERATIONS MEDICAL LEADERS HANDBOOK, 2024
iv NSO: NATO STANDARD ATrainP-5 LANGUAGE PROFICIENCY LEVELS, May 2016
v SHAPE Europe: ACO DIRECTIVE 080-101 PERSONNEL RECOVERY IN NATO OPERATIONS, April 2015
vi NSO: NATO STANDARD AMedP-1.6 Medical Evaluation Manual, September 2018
vii International Humanitarian Law Databases: Geneva Conventions, Article 40 (2), 2016
viii NSO: NATO STANDARD AMedP-1.8 Skills Matrix, January 2016
ix NSO: NATO STANDARD AMedP-8.5 MINIMUM TEST REQUIREMENTS FOR LABORATORY UNITS OF IN THEATRE MILITARY MEDICAL TREATMENT FACILITIES (MTFs), June 2023
Kommando Schnelle Einsatzkräfte Sanitätsdienst
OLt Frank Klemmer
SPOC SpezKrBw Kdo SES G3.2
Papenburger Sraße.82
26789 Leer
E-Mail: [email protected]