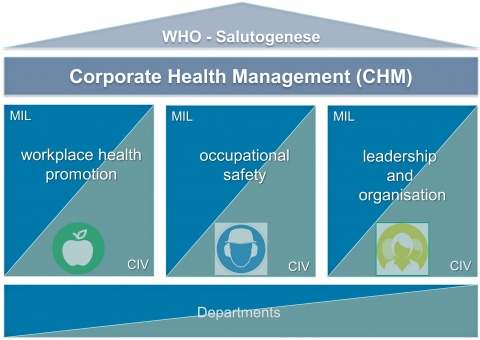
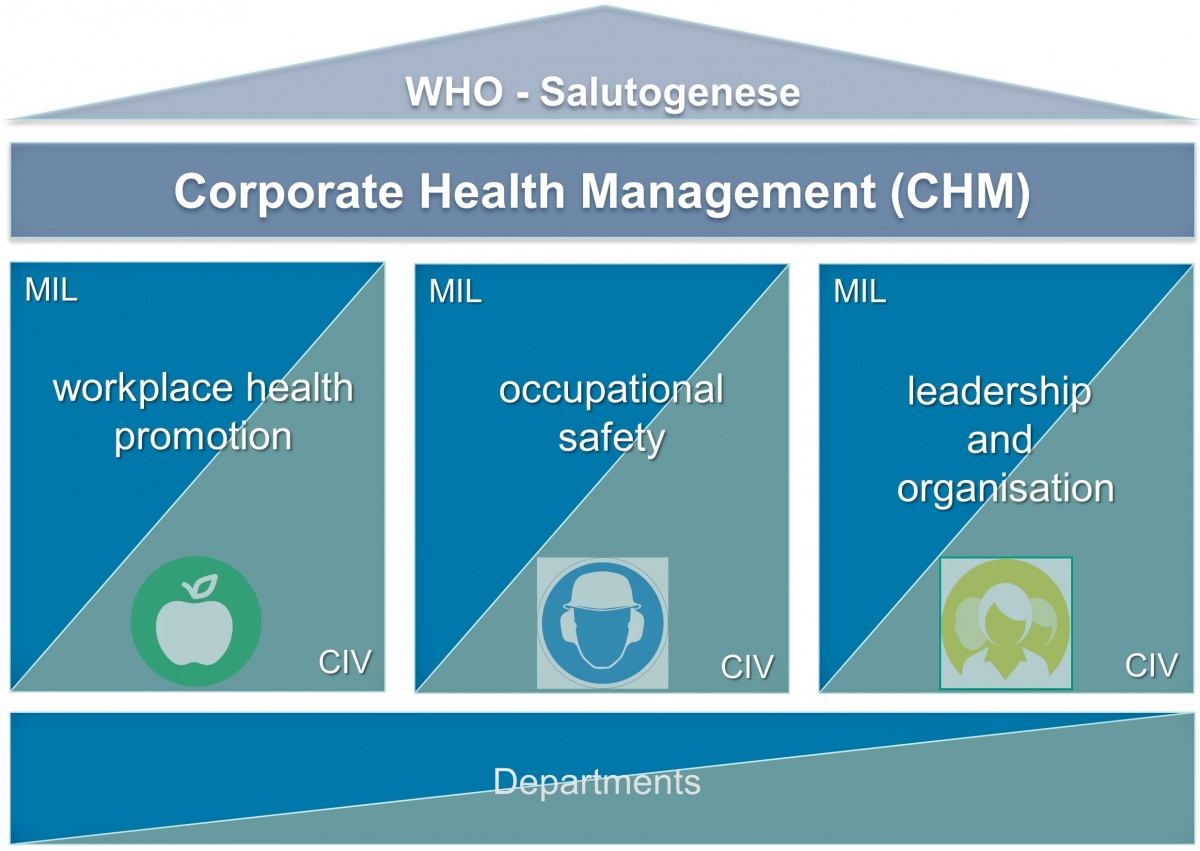
Figure 1: Corporate Health Management (CHM) in the responsibility of the Federal Ministry of Defence with the three main topics
Annika Claus¹, Dirk-Matthias Rose¹, Stefan Sammito²,³
The Federal Ministry of Defence (MoD) started the implementation of corporate health management (CHM) on January 1st 2016 after a pilot phase in 2015. At the end of the year 2019 CHM shall be implemented nationwide at all government departments of the MoD.
At the beginning in 2015 the evaluation phase starting with 10 military, civil, and medical agencies with different tasks and infrastructure had been scientifically accompanied and evaluated by 8 university and non-university research institutions. Aim was to customize the experiences with CHM in civil industry to the special needs of the Bundeswehr. An example of a successful transfer from civil research to an essential tool of military CHM is the web-based tool of an employee attitude survey AIGScreenBw. AIGScreenBw is currently used to survey the actual status of individually perceived work and health situation. On a long term, the tool will reevaluate the status of the agencies, especially after realized measures based on the results of the first survey.
AIGScreenBw has been developed from a survey to assess the individual health situation of teachers in Rhineland-Palatinate. The core questionnaire comprises several items covering the main aspects of the working conditions, individual´s health, and stress responses. Further questions concerning respective circumstances and demands were added to the AIGScreenBw such as attitudes towards CHM or socio-economic characteristics. Since 2015, the survey with total 134 items was evolved and can be used as a paper-pencil-version or as an online survey. Each agency can use this survey. The custom-tailored reporting will be retransmitted to the agency within few working-days including reference values from other agencies. To date (15th February 2019) 123 agencies with a total number of employees of 66,157 have been surveyed. The results in the topics “health promotion”, “safety and occupational health” and “organization and leadership” will be presented exemplary.
AIGScreenBw is a scientific developed tool for employee attitude surveys to verify the occupational strain at the workplace in the Bundeswehr. It is an ex-ample how to transfer knowledge from civil research to armed forces reasonable and cost-effective.
Keywords: Work place; leadership; health promotion; occupational safety
Das Bundesministerium der Verteidigung (BMVg) hat nach einer Pilotphase in 2015 am 1. Januar 2016 mit der Einführung eines Betrieblichen Gesundheitsmanagements (BGM) in allen Dienststellen im Geschäftsbereich des BMVg begonnen.
In der 2015 durchgeführten Pilotphase fand zunächst eine Evaluierung an 10 militärischen und zivilen Dienststellen mit unterschiedlichen Aufgaben statt. Diese wurde von acht universitären und nicht-universitären Forschungseinrichtungen wissenschaftlich begleitet. Ziel war es, Erkenntnisse aus zivilen BGM-Projekten an die Anforderungen und Besonderheiten der Bundeswehr anzupassen. Ein Beispiel für einen erfolgreichen Transfer stellt hierbei die Anpassung einer Mitarbeiterbefragung für das BGM der Bundeswehr dar. Diese als AIGScreenBw bezeichnete Befragung dient der Erhebung der jeweiligen Arbeitsplatzsituation und des Gesundheitsverhalten der Mitarbeitenden an einer Dienststelle. Im Rahmen einer Reevaluation dient die Mitarbeiterbefragung auch der Überprüfung der Wirksamkeit der durchgeführten BGM-Maßnahmen zur Verbesserung der Situation an der Dienststelle.
Die Mitarbeiterbefragung AIGScreenBw wurde aus einer Befragung für Lehrkräfte in Rheinland-Pfalz weiterentwickelt. Die Befragung umfasst Fragen zum Arbeitsplatz, individuellen Gesundheitsverhalten und -zustand und zu Stressreaktionen. Darüber hinaus werden Fragen zur eigenen Einstellung zu BGM-Maßnahmen, zur Bereitschaft zur Teilnahme und zu einigen sozio-ökonomischen Aspekten gestellt. Insgesamt umfasst der Fragebogen 134 Fragen und kann sowohl in einer Paper-Pencil-Version als auch in einer Onlinevariante durch einzelne Dienststellen der Bundeswehr durchgeführt werden. Eine dienststellenbezogene Auswertung wird der Dienststellenleitung zeitnah zum Ende der Befragung einschließlich entsprechender Referenzwerte übersandt. Mit Stand vom 15. Februar 2019 hatten 123 Dienststellen mit einer Gesamtzahl von 66.157 Mitarbeitenden an der Befragung teilgenommen. Beispielhaft werden im vorliegenden Artikel Ergebnisse aus den Bereichen „Gesundheitsförderung“, „Arbeits- und Gesundheitsschutz“ und „Führung und Organisation“ präsentiert.
Die wissenschaftlich entwickelte Mitarbeiterbefragung AIGScreenBw ist damit ein wesentliches Tool, um die Arbeitsplatzverhältnisse in der Bundeswehr zu ermitteln. Sie stellt gleichzeitig ein gelungenes Beispiel dar, wie wissenschaftliche Erkenntnisse von zivilen Forschungseinrichtungen effektiv und sinnvoll auf die Anforderungen in der Bundeswehr übertragen werden können.
Schlüsselworte: Arbeitsplatz; Führung; Gesundheitsförderung; Arbeitssicherheit
1.1 Legal obligation and economic necessity of Corporate Health Management
According to the German Occupational Health and Safety Act (ArbSchG), employers are obliged to contribute actively to the protection of the health of their employees through preventive measures. This includes the prevention of harm to health through the elimination of hazards at work, the implementation of concrete measures to protect and maintain the health of employees, and the identification and assessment of hazards to its employees. Furthermore, with regard to the measures taken, there is an obligation to review the effectiveness and, if possible, the optimization of these.
In addition to the legal obligation, it makes sense for employers to pursue health promotion and management from an economic perspective. A large number of studies confirm the economic benefits of corporate health management (CHM), both from an economic perspective and for companies. For example, Baicker et al. calculated in a meta-analysis that the average saving due to lost time exceeds healthcare spending by a factor of 2.7. Hochart et al. showed in a longitudinal analysis that health expenditure for participants in a health program increased by less than 1 % during the survey period, while non-participants increased their costs by around 22 % over the same period. Chapman & Larry described in his latest meta-analysis that the costs of occupational accident and disability insurance are reduced by an average of 25 % through occupational health promotion.
Simultaneously, new forms of stress, which are predominantly of a psychological nature, result from the change of requirement structures of work and the emergence of new forms of work, which are often associated with catchwords such as delimitation, flexibilization, service orientation, multitasking, or computeri-zation. The European Agency for Safety and Health at Work reports new forms of employment contracts and job insecurity, work intensification, a poor work-life balance, and high emo-tio-nal demands at work as the top emerging risks in the occupa-tio-nal context.
In addition, in view of an aging workforce structure in Germany, CHM is becoming an increasingly important topic for companies that want to maintain the working capacity of their employees for as long as possible and remain attractive as an employer for potential applicants.
A report by the Federal Institute for Occupational Safety and Health , however, already noted for 2012 a discrepancy between occupational medical care requirements and available capacities in Germany and predicted a further significant divergence in demand and supply. In order to counteract the increase in this gap, the use of demand-oriented management and planning as well as the use of already available resources in the company is recommended. Therefore, the Federal Institute for Occupational Safety and Health proposes a multidisciplinary approach as one way of optimizing the use of resources regarding occupational health and safety. With the involvement of internal and external actors, such as safety engineers, ergonomists, psychologists or statisticians or institutions like universities, occupational physicians can be relieved and concentrate more on their core task. By using expert knowledge of the various disciplines, synergy effects can be used that enable a more comprehensive knowledge of needs for action and a custom-made and holistic health management. This results in a demand-oriented solution which is more cost effective compared to a “one-fits-all” approach.
1.2 Pilot Project
The multidisciplinary approach was also applied in the pilot project to implement CHM in the area of responsibility of the MoD. This involved occupational physicians, heads of department, military psychologists, CHM coordinators and research partners from eight Universities and research institutes with a speciali-zation in epidemiology, social medicine, nutritional science, psychology, occupational health and safety, sports science, and survey methods.
CHM consist of „workplace health promotion” with the subtopics in “physical activity”, “nutrition”, “prevention of dependence” and “reducing of stress” and of “occupational safety issues” and the topic “leadership and organisation” (see figure 1).
The pilot project started in January 2015 at ten departments in eleven locations, which were considered to be representative for the organizational structure of all units. This includes the administration, represented by the Federal Ministry of Defence, the Federal Office for Human Resources, the Federal Office for Equipment, Information Technology and Use of the Bundeswehr and the Food Office, as well as units of the armed forces, represented by a corvette squadron, a grenadier battalion, an operations command, an electronic warfare battalion, and medical care unit, represented by the Bundeswehr Hospital Ulm.
During the pilot phase the CHM was accompanied by different research projects 7, 11, 13, 14, 23, 24]. These projects examined relevant subtopics in the field of intervention studies. Additionally a survey was needed to determine the situation in the different departments and for the area of responsibility of the German MoD with 250,000 employees in total. For this reason, it was necessary to gain information about the work situation, individually perceived work stress, health behavior of the em-ployees and their health situation as well as their needs. For this purpose, a questionnaire (“AIGScreenBw”) was developed and evaluated during the pilot phase.
1.3 Implementation phase
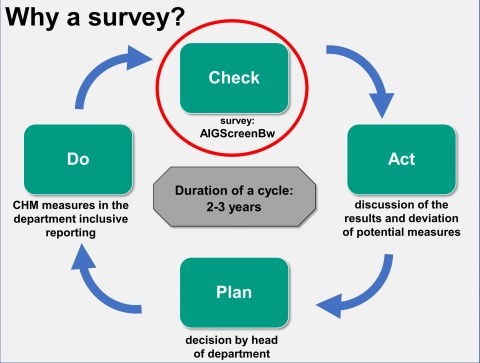
After a successful pilot phase the MoD decided to implemented CHM in all departments in the area of responsibility of the German MoD. Hence a CHM organisation was created at the beginning of 2016. Forty-four regional CHM coordinators were tasked to implement a CHM successively at the departments in their regional area. For this reason they gave advice to the unit commanders and the heads of departments. At the end of 2019 the implementation of CHM should be finalised at all departments.The employee´s survey AIGScreenBw should also be used for the implementation phase in dependence of methodical consideration of a PDCA cycle (see figure 2). Based on the survey during the pilot phase the items in the survey were adapted and since May 2017 an improved version (2.0) was used. By now the survey has 134 items according to the followed topics:
The survey is conducted primarily online. Only in departments where not all employees have a computer access or are not connected to the internet an additional paper-pencil survey can be used. With the exception of items from the Engagement Index and the socio-demographic items all items can be answered on a four-point-likert-scale. The answers are labelled with “no”, “rather no”, “rather yes” and “yes”.
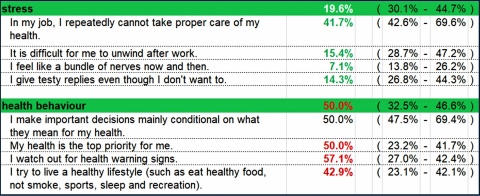
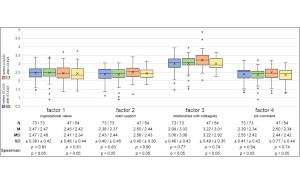
For each subject area an indicator is determined. It corresponds to the mean value of the percentages of personnel that have chosen answers from negative categories for the individual items of the subject areas. The range differs from 0 % (no negative associated answer over all separate items for this indicator) to 100 % (all answers are negative associated). While combining questions under one score leads to a reduction of the level of detail, it allows addressing various sub-aspects under one indicator. Indicators were checked for internal consistency (Cronbach‘s alpha 0.506-0.906).
Up to 15th February 2019, 123 departments with a total of 66,157 employees were queried. 17,667 employees took part in the survey (response rate 26.7 %).
Results from the survey where examined on department level and in addition on section or company level. The indicators are shown clearly in a One-Paper (see figure 3).
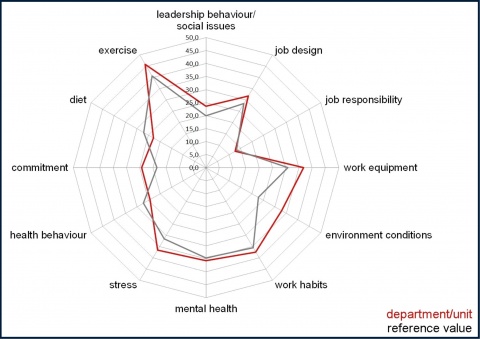
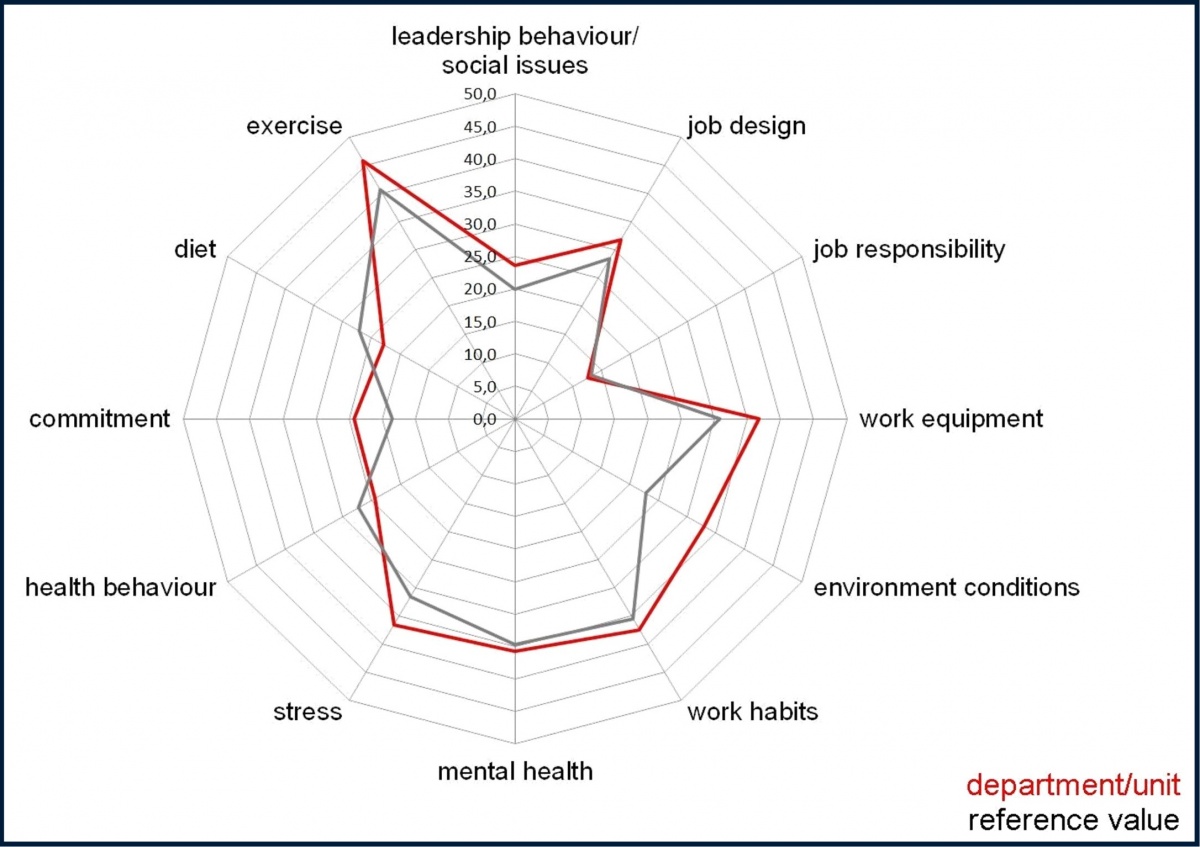
For comparison, reference values for every item and for the indicators were calculated as an average from the results done before. This is shown for every survey also in the results for the head of department (see figure 4).
Previous published analyses have pointed out that with this survey tool the different working conditions and loads can be captured delimitable. Analyses of the survey results of the pilot phase have shown, that in eleven of the twelve indicators there are significant differences between the departments with either belong to military command, or administration, or combat units or military hospital (see table 1).

A survey is one way for examination of working conditions and load of employees. Furthermore, there are additional possibilities for evaluating the needs for CHM measures. Analysis of response rate of employees for the CHM measures or an evaluation of singular measures in addition to the survey are two possibilities and preferable. It should be kept in mind that a survey also has some restrictions. Because the participation in the survey is on voluntary base the results could have some bias in comparison to the total group of employees in the department. Especially persons who are interested in the field of health and wellness would take part in such a survey. Thus, it is not surprising, that during the pilot phase women and civilian employees took part disproportionately more often in the survey than the group of men or soldiers. Since the measures during the pilot phase were focussing on exercise and health promotion items, participation especially for the group of civilian employees was very attractive because the evaluation was conducted during the normal working hours. For soldiers who were instructed to take part in the physical fitness training during normal duty exercise measures are less attractive. Keeping this in mind, it is surprising that the number of negative associated answers in the indicator of exercise is so high in combat units [8]. The high participation rate of women converges with the knowledge that women are more open minded for preventive medicine measure-ment that men.
During the implementation phase the response rate increased (26.7 % instead of 22.4 %). The goal of a survey should be a maximum recruitment of all participants. With the possibility of conducting the survey as a single online survey or as a combined online/paper-pencil survey it is possible to reach each employee in the different departments. This approach was chosen, because online survey have several benefits in comparison to other survey methods:
• economical with regard to time, material and personal needed,
• flexible with regard to time and location for the survey, and
• in addition, interviewer effects can be minimised through the automatically collection of the results.
Because not all employees in different departments had a computer access an additional paper-pencil survey had to be conducted. Questionnaire content, design and order were the same in both survey methods. So no additional effects were expected from this proceed. On the other site without an additional paper-pencil survey a lower response rate and a high selectivity of employees taking part in the survey would be expected.
Though, even with this measurement and a detailed information policy in the run-up of the survey (kick-off events, flyer, poster) only 26.7 % of all employees have taken part in the survey so fare. In comparison to other surveys in the field of CHM this value can be classified as low, e.g. Spegel et al. had shown a response rate in six Bavarian services of 34 to 60 %. On the other hand, Schmidt et al. got a response rate of 15.0 to 16.4 % in four hospitals while in a parallel survey in different services a response rate of 29.5 to 52.7 % could be reached.
The indicators were designed to get a maximum acceptance and comprehensibility in the target group of employees in the responsibility of the German MoD. Because of this an adapted questionnaire for the military context was used. On the other hand, there was a challenge to address all the different aspects of the broad area of indicators with regard to a CHM and to keep the questionnaire as short as possible. Because of this, there was only a small possibility to use validated questionnaires. For this reason a validation is planned and will be conducted in 2019/20.
In summary, the designed survey of the CHM in the responsibility of the German MoD can collect important information for planning target-oriented CHM measures. It supports the military commanders and the heads of departments in planning and tracking the working conditions and loads and the impact of the CHM in a PDCA cycle.
Acknowledgement:
The research project had been conducted on behalf and with approval of MoD (E/U2AD/HD003/HD001) and within a special research frame (research no.: 06KS-S-63 1619).
For the Authors:
M.A. Annika Claus
Institut für Lehrergesundheit am Institut für Arbeits-,
Sozial- und Umweltmedizin der Johannes Guttenberg-Universität Mainz
Kupferbergterrasse 17-19, 55116 Mainz
E-Mail: [email protected]
Als Vortrag gehalten beim STO-HFM-302 Symposium „Evidence-Based Leader Interventions for Health and Wellness“ in Berlin, 9. bis 10. April 2019; der Artikel wird zu einem späteren Zeitpunkt auch im Internet in den Educational Notes zum STO-HFM-302 Symposium (www.sto.nato.int) veröffentlicht werden.
Datum: 24.06.2019

Im Fokus der aktuellen Ausgabe steht das neue Kommando Unterstützung in Bonn und der Unterstützungsbereich der Bundeswehr. Traditionell behandelt die zweite Ausgabe des Jahres den Schwerpunkt…

Der militärische Such- und Rettungsdienst (SAR) der Bundeswehr spielt eine entscheidende Rolle bei der Durchführung von Rettungsaktionen im deutschen Luftraum und in angrenzenden Seegebieten. Die…

Das neue Unterstützungskommando wurde am 1. Oktober 2024 in Dienst gestellt und erreichte zum 1. April 2025 seine volle Einsatzbereitschaft. In diesem Exklusivinterview erläutert der Befehlshaber…

Ludwigshafen, 3. April 2025 – Vom 1. bis 4. April fanden an der BG Klinik Ludwigshafen die „Rhein-Neckar Tage für Medizinischen Katastrophenschutz“ statt. Im Fokus der Fachveranstaltung…

Eine bewegende Verabschiedungsfeier, die am 28. November 2024 im Offizierheim der Sanitätsakademie der Bundeswehr vor 120 geladenen Gästen stattfand. Anlass war die Versetzung in den Ruhestand von…

Im Rahmen der Informations- und Lehrübung Sanität im niederbayrischen Feldkirchen hat General Dynamics European Land Systems (GDELS) am 4. Juli das mittlere geschützte Sanitätsfahrzeug…

Die aktuelle außen- und sicherheitspolitische Landschaft ist von vielschichtigen, dynamischen und oft unvorhersehbaren Herausforderungen geprägt – von hybriden Angriffen wie Cyberattacken bis hin…

Am 19. Mai übergab Generalarzt Dr. Jürgen Meyer in seiner Funktion als Chef des Stabes beim Kommando Gesundheitsversorgung der Bundeswehr die Leitung über das Multinational Medical Coordination…

Die Grenze der Auflösung eines konventionellen Lichtmikroskops wird bei einer 1000-fachen Vergrößerung erreicht. Die Verwendung von Elektronenstrahlen und Magnetspulen als Linsen – das…

Nur 17 Monate nach Vertragsschluss hat das Beschaffungsamt der Bundeswehr gestern zwei neue, hochmoderne Sanitätscontainer vom Auftragnehmer übernommen, die über die Logistik des…


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}