Results of a prevalence study of the US-Army [14]
Stefan Sammito¹,² and Lisa Müller-Schilling², ³
Objective: The purpose of basic military training (BMT) is to enable recruits to acquire basic military skills and develop the required physical fitness. This training is accompanied by increased physical strain and the risk of injury and excessive stress symptoms (I&ESS). The objective of this study was to examine the extent to which the level of physical fitness at the beginning of basic military training affects the incidence of I&ESS and resultant absences from duty.
Method: The data of a total of 774 male subjects (age 20.5 ± 2.2 years) from 8 subsequent BMT quarters was analysed. The medical diagnoses made during the consulting hours of the unit physicians were reviewed for I&ESS and the kinds of injuries incurred as well as the sick leave pronounced were documented. The level of physical fitness per quarterly period was categorised by means of the total numbers of points achieved during the standard basic fitness test (BFT). This categorisation was finally used as a basis for an analysis of the lost days in relation to the level of physical fitness.
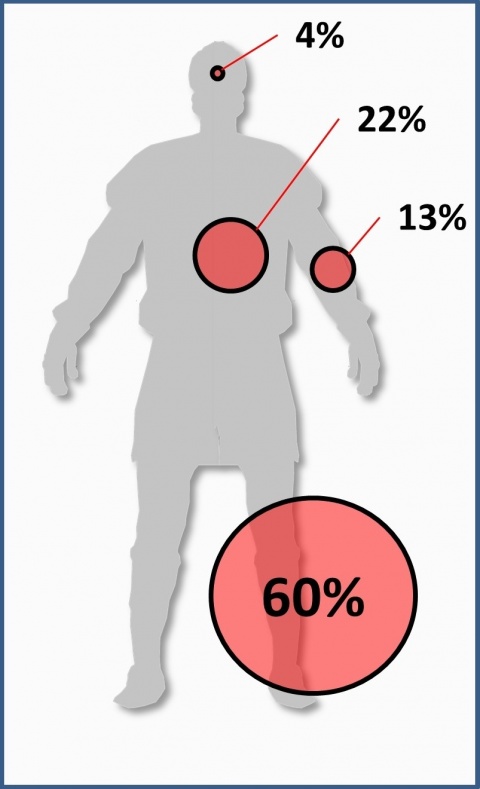
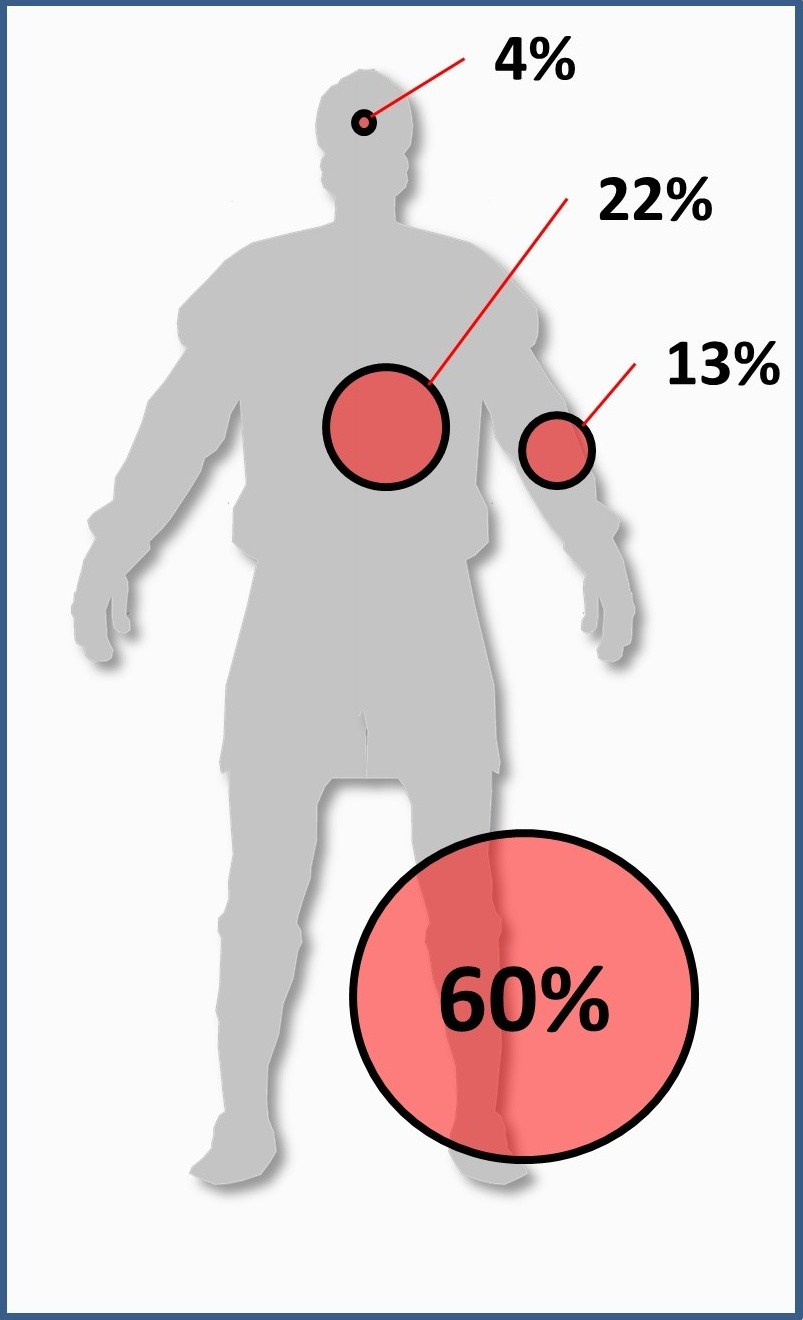
Results: In total, 255 of 774 subjects (32.9%) reported to the unit physicians with I&ESS. 60% of all the injuries were lower extremity injuries. There was a significant increase in the length of absence from duty among the group with the lowest level of physical fitness.
Conclusions: The analysis revealed that the level of physical fitness at the beginning of BMT has a significant influence on the length of absence from duty due to I&ESS. The high percentage of lower extremity injuries shows the specific relevance of a reduction of I&ESS to avoid limitations during BMT which otherwise may occur.
Keywords: Military, injury, training, excessive stress symptoms, physical fitness
In addition, the increasing lack of exercise among juveniles and young adults results in a reduction in physical resilience among potential first-time employees [7, 11, 20]. Employees are especially unable to reliably perform complex activities like those mentioned above when they take up a new occupation. This is why first-time employees in the military initially undergo several months of BMT. Injuries and excessive stress symptoms (I&ESS) during BMT can reduce the time available for training and thus its overall quality significantly. American and Israeli studies have isolated various risk factors that influence the incidence of I&ESS during basic combat training (BCT) [1, 2, 4, 12, 17, 21, 22, 25, 26, 27]. Besides other risk factors, such as being female [17, 21] underweight or overweight [4, 12], a smoker [5, 17, 19], of a certain age [12, 19] or belonging to a specific ethnic group [5, 12, 19, 26], physical fitness at the beginning of the training period has been revealed to be a key predictor.
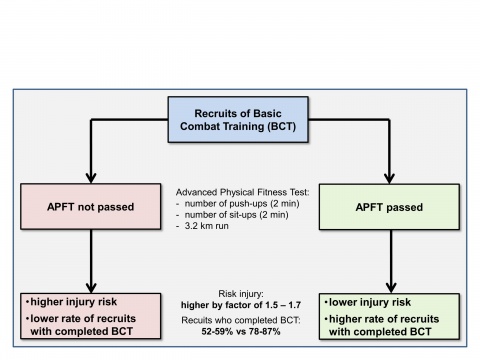
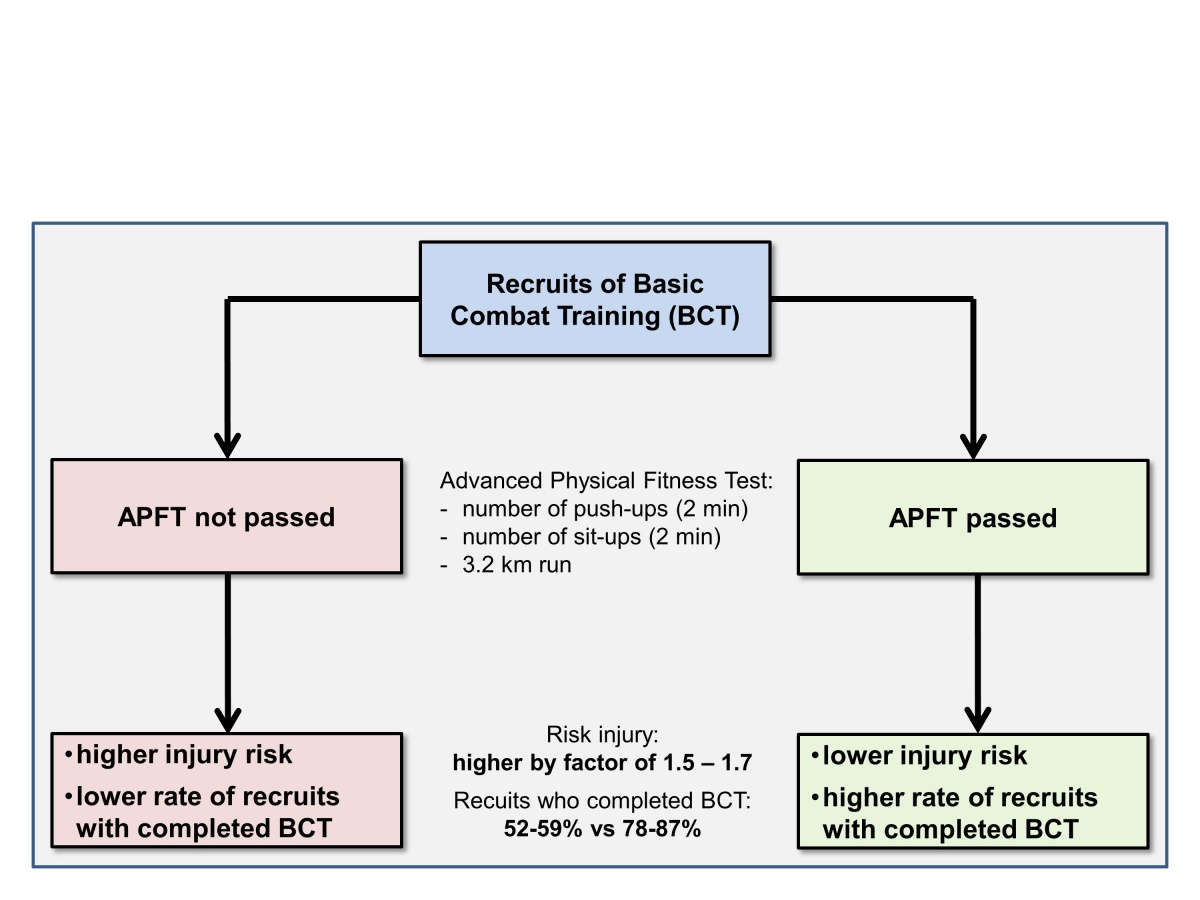
Findings of the US armed forces show examples of how we can handle this modifiable risk factor in terms of a prevention strategy with, at the same time, better performance of course-related tasks. It was found out that US Army recruits were more likely to get hurt during Basic Combat Training (BCT), by a factor of 1.5 to 1.7, when they had not passed the initial Advanced Physical Fitness Test (APFT). Furthermore, the rate of recruits without passing initial APFT who finalised the BCT (52 % to 59 %) was lower than of those recruits who had passed the initial APFT (78% to 87%) [14] (see Figure 1). After the introduction of an eight-week pre-fitness training for recruits who had not passed the APFT with the overall objective of integrating them into BCT until the end of this pre-training, the risk of injury could be lowered significantly and, at the same time, the rate of recruits who successful finalised the BCT could be improved in an impressive way - from 59% to 83% with male recruits and from 52% to 69% with female recruits [14].
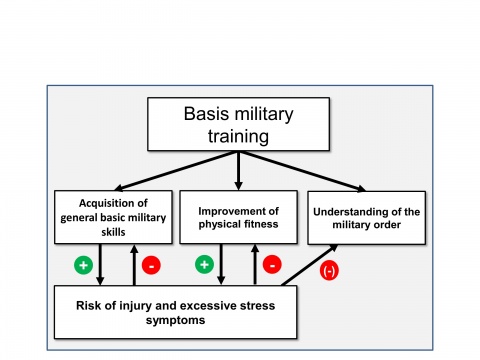
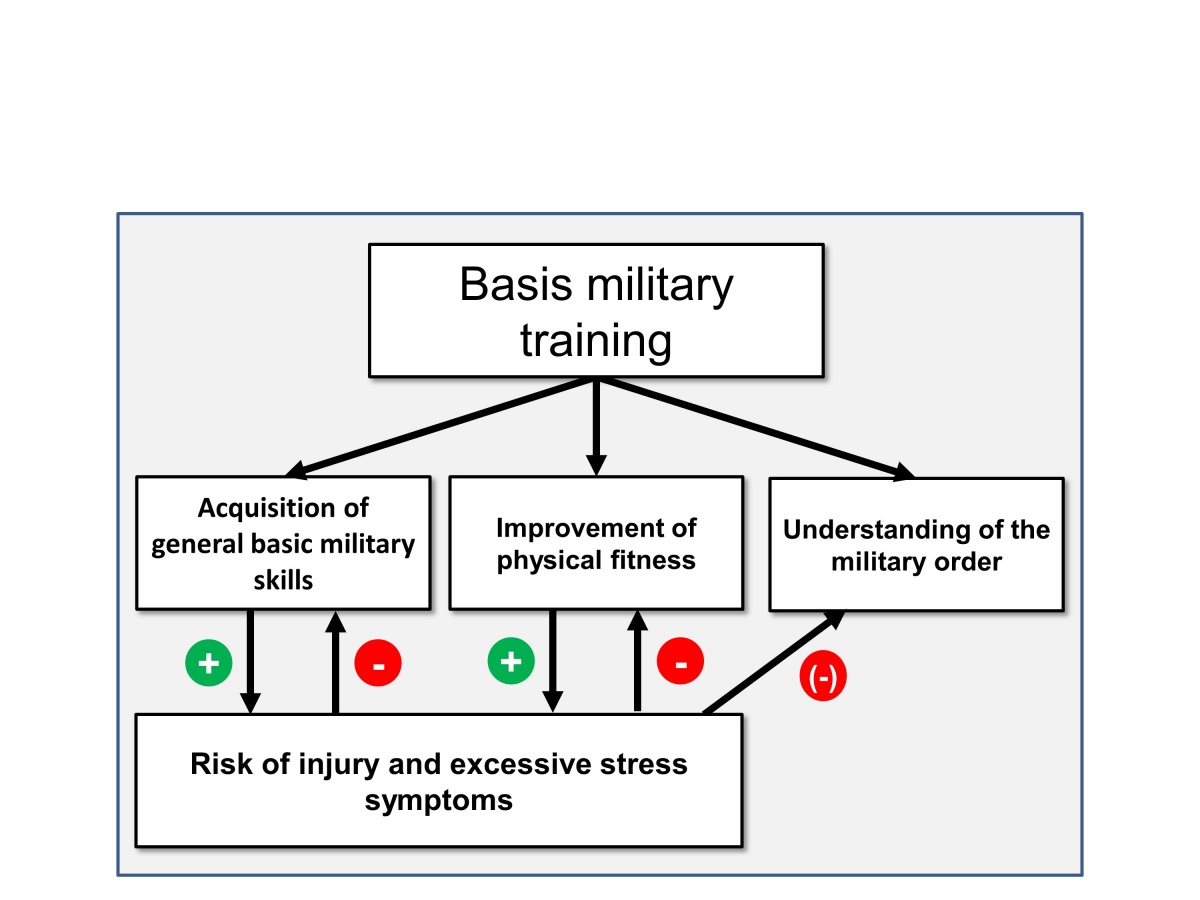
Using a model, the objective of BMT can be summarised in a simplified way in three factors:
The first two objectives especially increase the risk of I&ESS, which in turn as a negative feedback due to lost days have an adverse effect on the achievement of the BMT objectives (see Figure 2).
The primary objective in this regard should be to plan and carry out training periods for the improvement of physical fitness and for the acquisition of general basic military skills in such a way that, on the one hand, the training objective can be reached, but, on the other hand, the strain on the recruits is such that the risk of I&ESS is reduced.
Unfortunately, the findings of the working group led by KNAPIK et al. cannot be directly applied due to the above-mentioned differences between the US armed forces and the Bundeswehr. However, the incidents that happened in summer 2017, especially in the officer candidate battalion in Munster, show the importance of a scientific discussion of this topic.
The objective of this study was therefore to determine the influence of the initial level of fitness of recruits on the incidence of I&ESS during BMT in the Bundeswehr.
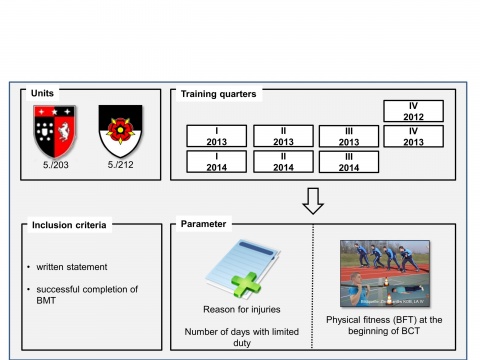
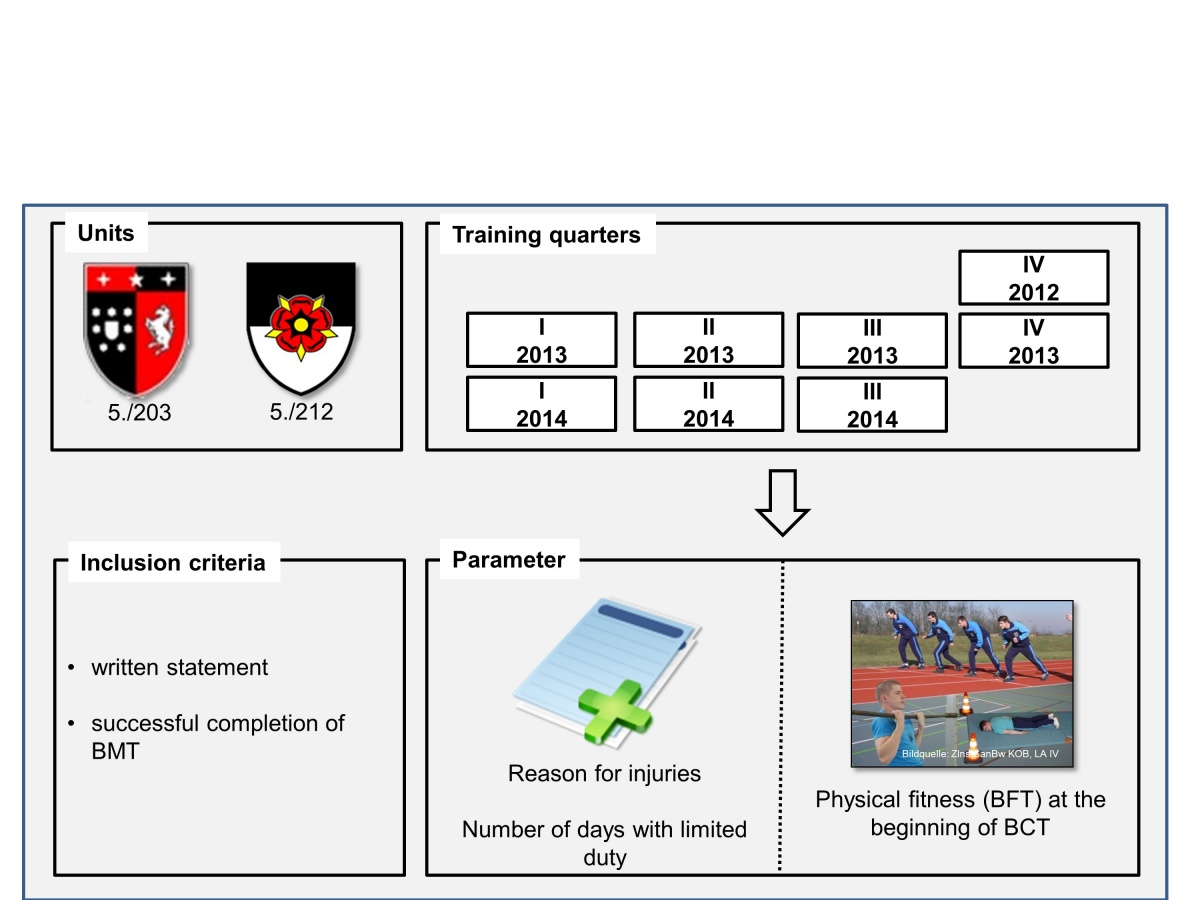
Two criteria for inclusion in the study were the successful completion of BMT and the issue of a written statement confirming that participation in the study was voluntary. In total, 774 subjects (age 20.5 ± 2.2 years, body-mass index [BMI] 23.5 ± 2.8 kg/m²) were included in the study. This means that 67 % of all the recruits undergoing their BMT during that period took part in it. There were no significant differences in the ages and body measurements of those who participated in the study and the recruits who did not participate (see Table 1). Table 2 shows the various quarters and training companies to which the participants were allocated.
Table 1: Comparison of the anthropometric data of those who participated in the study and those who did not
Participants | Non-Participants | P | |
Number | 774 | 383 | |
Age [years] | 20.5 ± 2.2 | 20.6 ± 3.2 | 0.883 |
Body height [cm] | 179.6 ± 7.0 | 179.2 ± 6.6 | 0.437 |
Body weight [kg] | 75.9 ± 11.2 | 76.6 ± 10.4 | 0.418 |
BMI [kg/m²] | 23.5 ± 2.8 | 23.8 ± 2.7 | 0.079 |
The medical data were reviewed for periods of absence from duty due to I&ESS, and the periods were documented. As a specific military feature, periods of full administrative leave were documented (in the civilian health system, such leave corresponds to a general inability to work) alongside periods of limited fitness for duty (e.g., exemption from outside duty activities, marching, physical training or field duty).
Table 2: Allocation of participating recruits to the various quarters and training companies with the respective total numbers of all the recruits trained during this quarter, 5./203 = Tank Battalion 203 training company, 5./212 = Armoured Infantry Battalion 212 training company
Quarter | 5./203 | 5./212 |
IV/2012 | 53 / 105 (50%) | 119 / 133 (89%) |
I/2013 | 39 / 69 (56%) | 71 / 81 (88%) |
II/2013 | 51 / 65 (78%) | 40 / 55 (73%) |
III/2013 | 57 / 123 (46%) | 37 / 56 (66%) |
IV/2013 | 64 / 121 (53%) | 66 / 94 (70 %) |
I/2014 | 53 / 74 (72%) | 44 / 53 (83%) |
II/2014 | No BMT | 29 / 58 (50%) |
III/2014 | 51 / 70 (73%) | No BMT |
Total | 368 / 627 (59%) | 406 / 530 (87%) |
Sub-analysis groups were defined for I&ESS that were attributed to general military training in the field, obstacle course training, self-protection training in CBRN hazard situations, marksmanship training (all four categorised as general military training) and mandatory physical training. Acoustic trauma incurred during marksmanship training and blisters incurred during marches were excluded.
The initial level of physical fitness was documented on the basis of the BFT results [6, 20]. This standard test consists of an 11 x 10-metre sprint, a flexed arm hang and a 1000-metre run and is always conducted at the beginning of BMT. Based on the BFT results of 719 recruits, fitness levels were categorised by quartiles, and the lost days due to I&ESS within each quarter were then analysed by means of ANOVA and a subsequent Dunnett-T post-hoc analysis. Furthermore, the I&ESS were analysed with regard to the body regions affected and their incidence during the various kinds of training. For the exposition analysis, the numbers of I&ESS were put into relation with the periods of exposure. The calculations of the periods of exposure were based on the number of hours for which each kind of training was scheduled to be conducted in the duty rosters, and lost days due to illness were factored in for each recruit.
This study was approved by the ethics commission of Otto-von-Guericke-University Magdeburg (file no: 111/12).
During the study and in consideration of the fitness for duty of the participants, a total of 283,831.1 hours of general military training were conducted, the largest share of which was assigned to marksmanship training (138,082.3 hours) and field training (134,411.4 hours). Obstacle course training (5,446.1 hours) and CBRN defence training (5,891.3 hours) constituted only a minor share of the training time. Mandatory physical training, amounting to 18,959.8 hours, also only made up a rather small part of the total time for BMT. The time each recruit spent on training was 178.4 hours for marksmanship training, 173.7 hours for field training, 7.6 hours for self-protection training in CBRN hazard situations, 7.0 hours for obstacle course training and 24.5 hours for mandatory physical training.
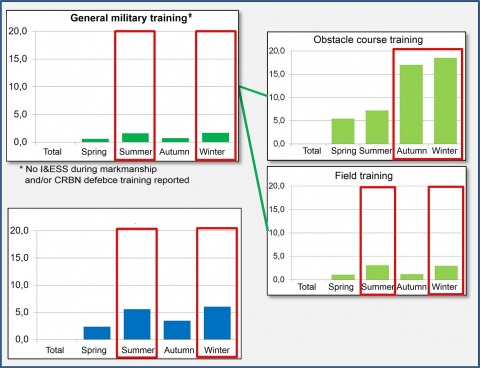
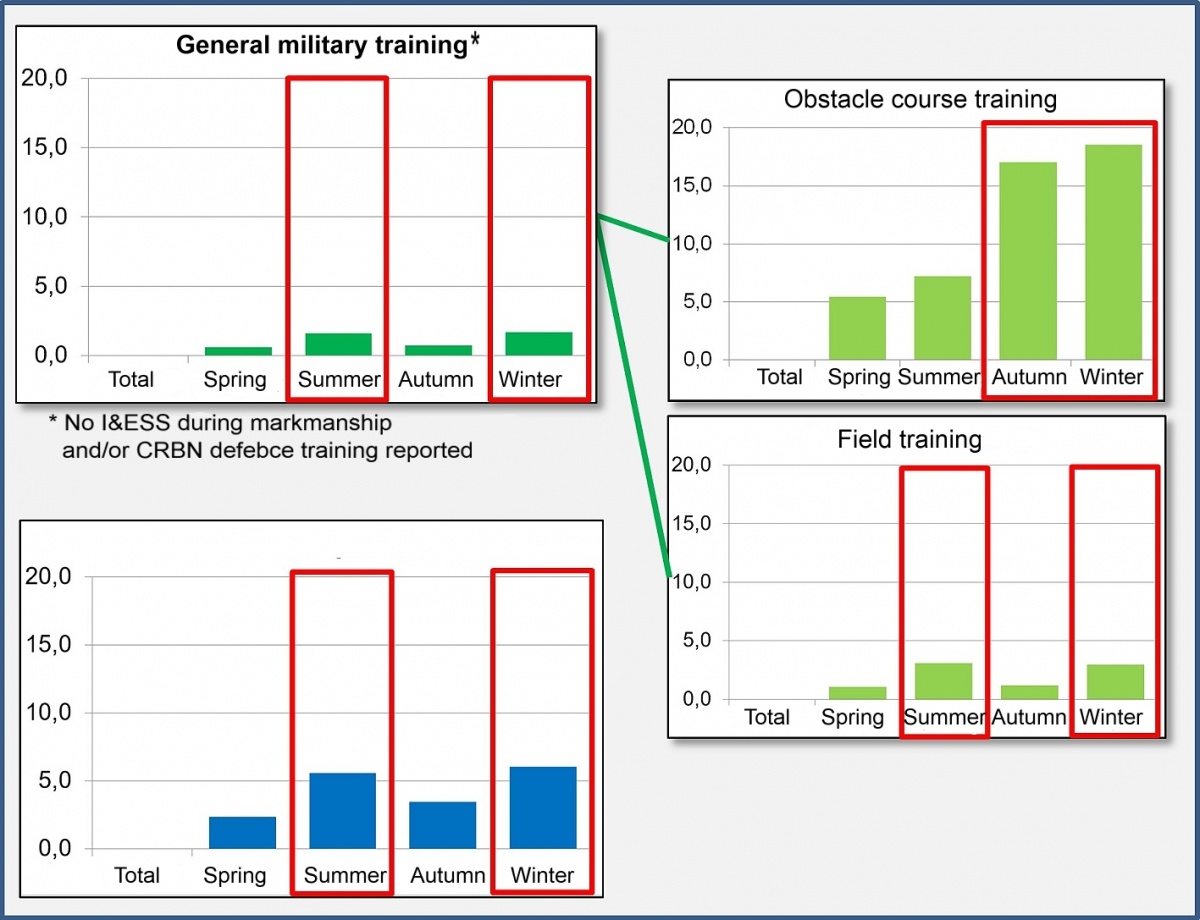
The analysis of I&ESS cases per 1,000 hours of specific training showed an incidence of 1.09 I&ESS/1,000 hours during general military training and 4.17 I&ESS/1,000 hours during mandatory physical training. A sub-analysis of the incidence of I&ESS during general military training, which comprised marksmanship training, CBRN defence training, obstacle course training and field training, revealed that a high number of I&ESS were incurred during obstacle course training, while no cases were incurred during marksmanship and CBRN defence training (see Figure 5). An increase in the number of I&ESS was also observed during the summer and winter quarters, especially as a result of field training and mandatory physical training (see Table 3).
The ANOVA analysis revealed that physical fitness had a significant influence on the length of absence from duty in association with the total number of lost days due to I&ESS. The average number of lost days was significantly higher in the quartile with the lowest level of fitness than in the other quartiles (see Table 4).
Compared to data collected in 2008/9 [24], BMT in its present form is estimated to cause substantially less injuries, since a decrease in the average number of injuries from 2.27/1,000 hours to 1.45/1,000 hours has been documented. This is probably largely due to the implementation of a new marksmanship training concept in BMT. This concept provides for a significantly higher number of training hours on the ranges, with the result that the number of hours set aside for field training has been reduced and reallocated for marksmanship training, during which particularly few injuries are caused and hence less I&ESS are incurred on the whole. This was also revealed by the data analysis.
This study has shown that general military training was the main cause of injuries (57 % of all injuries). Considering the high total number of training hours, however, the incidence of injuries per 1,000 hours, with the average being 1.09/1,000 hours, is rather low. Moreover, the division of general military training into four sub-categories reveals that there are training-specific differences involving varying risks of injury. Marksmanship and CBRN defence training have proved to cause particularly few injuries, with no I&ESS having been found to be incurred from it. In contrast, at more than 18 I&ESS/1,000 hours in the winter quarters, the very high injury rate for obstacle course training stands out. Measured against the low number of hours allocated for obstacle course training, however, the injuries incurred in winter carry considerably less weight in the overall analysis. Even if a reduction in the high injury rate makes sense from the preventive medicine point of view, the obstacle course is a particularly good form of training for various movement sequences that are specifically required in military operations. What is important in this context is to weigh the physiological advantages offered by the specific training against the high injury rate.
Furthermore, an increase in I&ESS was noted during individual quarters. It is conceivable that this was due to the weather, as the influence of the weather on the surface conditions has already been identified as a cause of an increased injury rate during mandatory physical training in a study on injuries incurred during mandatory physical training at the same base [8]. Since general military training for the most part takes place outside, it is likely that (weather-related) changes in surface conditions in the winter months (due to snow and ice) and the summer months (highest precipitation rates of the year) may also be the reason for an increase in the risk of injury. The high number of I&ESS noted during the summer months can also be ascribed to other climatic conditions, such as the effects of higher temperatures on the body, which speed up the rate at which recruits become exhausted and increase the risk of injury, as found among recruits in the US military [13].
The analysis furthermore showed that the level of fitness of the recruits at the start of BMT had a significant influence on the incidence of I&ESS. The overall number of lost days for recruits with the lowest level of fitness was significantly higher than that for recruits with a higher level of fitness. The increase in the overall number of lost days also resulted in a loss of training time, and this clearly hampers the progress made in training by individual recruits. Moreover, lost days must be expected to lead to a further lowering of a recruit's level of fitness (at that time) and, in turn, an increase in the risk of their incurring (additional) I&ESS. This can lead to a further rise in the difference in physical fitness between recruits who incur injuries and others who do not lose days.
This result tallies with the findings of the US armed forces [14, 17]. To reduce the incidence of I&ESS, the level of fitness of recruits was raised by putting them through pre-training, and this significantly lowered the incidence of injuries during BCT [14, 15]. It can be assumed that this would also be the case with Bundeswehr recruits.
A pilot project of the German Army aiming at an adjustment of BMT which was launched with the Training and Support Company of Armoured Infantry Battalion 401 in Hagenow in the summer of 2018 has already taken up certain aspects of this idea. Instead of introducing pre-training, however, the percentage of physical training has been increased and concentrated within the first six weeks of basic training. By dividing recruits into performance groups, their different levels of physical fitness are taken into account. The goal is for all recruits to reach a minimum grade of 4 in the BFT conducted after the first six weeks of training so that they can all embark on the next training phase, which has its focus on general military training. This pilot run was scientifically supported by the Bundeswehr Institute of Preventive Medicine.
The results of the pilot phase support the approach pursued to date and they show how the physical fitness of recruits can be improved by adjusting the training [10]. The introduction of these new standards in all training facilities of the Bundeswehr Army [18] is thus a logical and consistent step with a view to improving the physical fitness of recruits and reducing I&ESS at the same time.
References
Conflicts of interest
The authors declare that there are no conflicts of interest with regard to the guidelines of the International Committee of Medical Journal Editors.
Citation mode:
Sammito S, Müller-Schillig L: Physical Fitness as a Predisposing Factor for Injuries and Excessive Stress Symptoms during Basic Military Training. Wehrmed Mschr 2019; 63(2): 34-39.
For the authors
Lieutenant Colonel Assistant Professor Dr. Stefan Sammito
Bundeswehr Medical Service Headquarters
Von-Kuhl-Straße 50, 56070 Koblenz, Germany
E-Mail: [email protected]
* This study contains data and results from the doctoral thesis by Mrs Müller-Schilling at the Medical Faculty of Otto-von-Guericke-University Magdeburg.
Datum: 21.03.2019

In Feldkirchen zeigt der Sanitätsdienst seine Leistungsfähigkeit bei der medizinischen Versorgung von Verwundeten. Bei der Informations- und Lehrübung des Sanitätsdienstes der Bundeswehr 2025…

Der moderne Anästhesist ist heute ein interdisziplinär tätiger Akteur in der prähospitalen, klinischen und postklinischen Patientenversorgung. Insbesondere im militärischen Kontext nimmt er als…

Heute hat der Beauftragte PTBS im Verteidigungsministerium, Oberstarzt Prof. Dr. Peter Zimmermann die Infokampagne "Angehörigenfragebogen PTBS" gestartet.

Die gezielte Entwicklung von körperlicher Leistungsfähigkeit und Belastungsresilienz ist essenziell für den Aufbau kriegsfähiger Streitkräfte. Besonders relevant erscheint dahingehend die…

Aufgrund neuer ziviler Regularien wandelt sich die onkologische Medizin in Deutschland. Mindestmengenregelungen, zunehmender Druck zur Zertifizierung und derzeit noch unklare…

Bei militärischen Einsätzen im Ausland kann es zu schweren Erkrankungen und Verletzungen kommen, die dazu führen, dass Soldaten und Soldatinnen zur weiteren medizinischen Versorgung repatriiert…
Lungenkrebs ist weltweit nach wie vor die häufigste krebsbedingte Todesursache und geht mit hoher krankheitsbedingter Morbidität einher. Aufgrund der uneinheitlichen und oft spät auftretenden…

• Ein Lehrstuhl auf dem Firmengelände – und ein Meilenstein für Forschung, Lehre und Innovation im Schulterschluss mit der Industrie • Das Institut für Medizintechnik und Elektrotechnik…
Irregular warfare disrupts conventional medical evacuation, requiring prolonged casualty care with limited resources. Damage control resuscitation, mobile surgical platforms, and prehospital…

Blut und Blutkomponenten sind eine limitierte, jedoch unverzichtbare Ressource in der medizinischen Versorgung – sowohl im zivilen als auch im militärischen Kontext. NATO-Hochrechnungen für den…
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}